Trump has begun another trade war. Here's a timeline of how we got here
Trump has begun another trade war. Here's a timeline of how we got here
 Canada's leader laments lost friendship with US in town that sheltered stranded Americans after 9/11
Canada's leader laments lost friendship with US in town that sheltered stranded Americans after 9/11
 Chinese EV giant BYD's fourth-quarter profit leaps 73%
Chinese EV giant BYD's fourth-quarter profit leaps 73%
 You're an American in another land? Prepare to talk about the why and how of Trump 2.0
You're an American in another land? Prepare to talk about the why and how of Trump 2.0
 Chalk talk: Star power, top teams and No. 5 seeds headline the women's March Madness Sweet 16
Chalk talk: Star power, top teams and No. 5 seeds headline the women's March Madness Sweet 16
 Purdue returns to Sweet 16 with 76-62 win over McNeese in March Madness
Purdue returns to Sweet 16 with 76-62 win over McNeese in March Madness

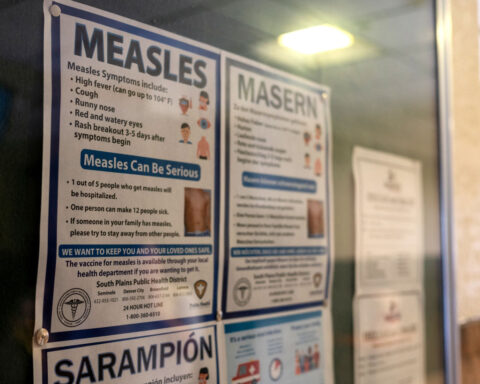
Modern evidence increasingly challenges long-accepted baselines about “normal” human body temperature established over 150 years ago. Recent studies of large populations find average readings substantially lower than the near-universal 98.6 Fahrenheit etched into medical lore. That leaves unsettled debates around properly identifying fevers amid shifting data that both reveals we run cooler today and highlights natural individual variations. With core measures declining below standardized cutoffs, some propose personalizing fever benchmarks while others argue widening diagnosis criteria risks overlooking serious infection.
The new normal results prime modern medicine to revisit physiological assumptions rooted in a different era. In the late 1860s, German physician Carl Wunderlich analyzed over a million temperatures to peg 98.6 degrees as typical. After tabulating his many readings ranging between roughly 97 and 100 degrees Fahrenheit, that number represented the midpoint - thus cementing 98.6 in medical consciousness for generations. Authoritative claims followed labeling temperatures up to 100.4 as consistent with everyday fluctuations but beyond indicating likely fevers. However, present research compiling big datasets consistently finds average readings nearly a full degree lower across genders, geographies and measurement methods today.
That consistent cooling trend spurs debate on its undercurrents alongside implications for clinical practice if almost 99 degrees worrisomely overstates current norms. Some posit that nineteenth century patients likely carried more inflammation, infection and dental issues slightly elevating their temperatures. Modern health gains like antibiotics that quell hidden bodily fires may shave degrees off population baselines over time. If so, losing a smidge of heat signals positive progress more than concerning decline or inaccuracy.
But measurement discrepancies between old thermometers and electronic monitors could also explain dropping data. Comparing historical readings based on device dissimilarities and collection inconsistencies proves hypothetical at best. With no directly relatable control groups over centuries, perhaps the most famous temperature statistic says more about lasting foundational citation than physiological shifts. Although a cooling trend remains biologically plausible for now, many view citing progress as speculation atop debatable data.
Still, experts agree continuing to rigidly teach nearly 99 degrees as average badly misrepresents current reality. A range gives needed latitude for variables like time of day, gender, or age instead of universal static figures. Younger women run hotter than older men, while everybody peaks later in afternoons - so no lone standard applies broadly. Even beyond those stratifying predictors, individuals demonstrate intrinsic setpoint diversity. Like heart rate or blood pressure, temperature varies within health, necessitating personalized baselines before defining deviations.
But therein seeds dispute on redrawing upper fever thresholds if “normal” slides nearer 97 than 98 degrees. Should 100.4 alarm points dip accordingly to catch mild but meaningful individual elevations? Some doctors warn against lowering goalposts that could muddle diagnoses and overlook Brewing illness. Slight upticks might escape notice if customary clinical cutoffs shift from entrenched precedent. In these views, widening normal bands matters more than moving fever fences barely maximizing sensitivity.
Others counter that subtler temperature bumps often escape detection in cooler patients today, risking lost early warnings. They advocate baseline personalization adjusted to each body’s habitual regulation patterns regardless of population figures. Under that model, today’s 98.6 already indicates possible brewing issues in some contexts absent other signals – demanding greater nuance incorporating clinical subtleties beyond blanket numbers.
In all scenarios, the emerging imperfections around statistical averages argues for balancing patient-specific clinical pictures instead of overreliance on isolated metrics. Doctors underscore interpretation art blending objective indicators and subjective reports, not magical cutoffs divorced from circumstances. Even fever proves just one useful puzzle piece for assembling diagnoses, not definitive threshold separating wellness from woe. Perhaps refocusing on holistic analysis helps modern practitioners emphasize deeper investigation skills withstanding evidentiary shifts.
While the field moves towards patient-centered care, recalibrated standards could better reveal individual insights against the thrum of human variability. But first medicine must reorient assumptions calibrated to previous knowledge bases before choppy waters between old habits and new realities. In the body’s intricate symphonies, measures once fixed turn fluid across eras and environments. Yet through acknowledging complexities and unknowns, diagnosis art persists helping make sense of changing states in systematic context. What endures remains practitioner wisdom humbly integrating objective indicators to grasp whole patient truths.