Trump has begun another trade war. Here's a timeline of how we got here
Trump has begun another trade war. Here's a timeline of how we got here
 Canada's leader laments lost friendship with US in town that sheltered stranded Americans after 9/11
Canada's leader laments lost friendship with US in town that sheltered stranded Americans after 9/11
 Chinese EV giant BYD's fourth-quarter profit leaps 73%
Chinese EV giant BYD's fourth-quarter profit leaps 73%
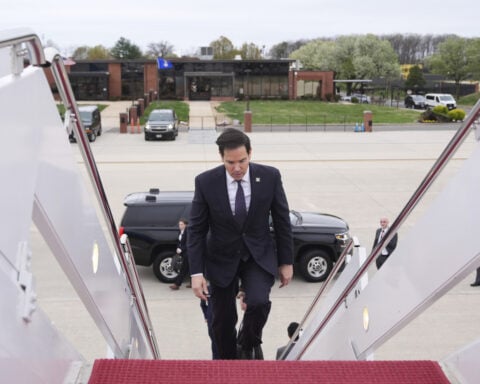
 You're an American in another land? Prepare to talk about the why and how of Trump 2.0
You're an American in another land? Prepare to talk about the why and how of Trump 2.0
 Chalk talk: Star power, top teams and No. 5 seeds headline the women's March Madness Sweet 16
Chalk talk: Star power, top teams and No. 5 seeds headline the women's March Madness Sweet 16
 Purdue returns to Sweet 16 with 76-62 win over McNeese in March Madness
Purdue returns to Sweet 16 with 76-62 win over McNeese in March Madness
Local|News
Swatting calls spark fear, massive police responses in California
False emergency reports, known as "swatting," are triggering massive law enforcement responses and causing widespread panic across California.
In early March, Claremont McKenna College experienced the consequences of swatting when a 911 caller claimed to be holding someone captive in a campus restroom. "The caller told dispatch they were in a restroom on the Claremont McKenna College campus, holding someone captive and threatening to harm them," the Claremont Police Department said in a statement. "They also stated they had a bomb and were going to walk around with a rifle and shoot anyone